
















Obesity vs. True Gynecomastia: How Doctors Diagnose It
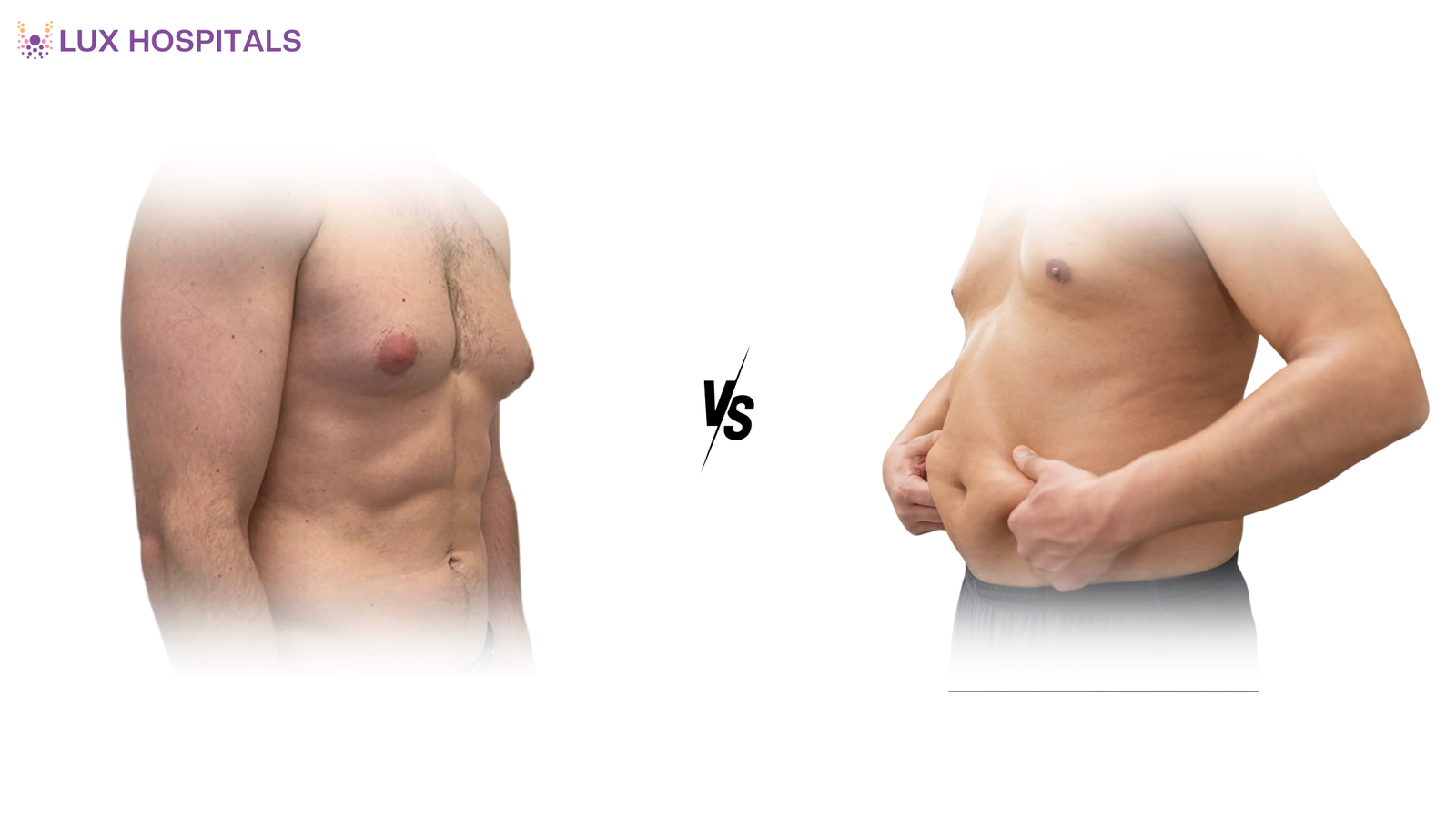
Many men feel embarrassed about chest enlargement. However, understanding the difference between obesity and true gynecomastia is the first step toward proper treatment. While both conditions cause an enlarged male chest, their causes, structure, and treatment plans are completely different. Doctors often see patients confused about whether they have excess fat due to weight gain or gland enlargement due to a hormonal imbalance. If you notice persistent chest enlargement, do not self-diagnose. Seek medical evaluation early.
What is Obesity-Related Chest Enlargement?
In Obesity vs. True Gynecomastia, obesity-related enlargement results from excess fat accumulation in the chest. This condition is sometimes called pseudogynecomastia. When body fat increases, fat cells store excess energy throughout the body, including the chest. The tissue feels soft and evenly distributed. Weight loss, exercise, and lifestyle changes often significantly improve this condition.
Key Signs of Obesity-Related Chest Enlargement:
- Soft, fatty chest tissue
- Associated with overall weight gain
- Improves with diet and exercise
- No firm gland under the nipple
Lifestyle modification is usually the first step in treatment.
What is True Gynecomastia?
In Obesity vs. True Gynecomastia, true gynecomastia involves enlargement of the male breast gland tissue due to hormonal imbalance. It commonly occurs during puberty, ageing, medication use, or medical conditions affecting testosterone and estrogen levels.
Unlike fatty tissue, glandular tissue feels firm or rubbery under the nipple. Exercise alone cannot reduce it. True gynecomastia may cause tenderness or psychological distress.
Common Causes:
- Hormonal imbalance
- Steroid use
- Certain medications
- Liver or thyroid disorders
A medical evaluation is necessary to confirm the diagnosis.
Obesity vs. True Gynecomastia: Key Differences
Understanding the difference between Obesity and True Gynecomastia helps patients choose the right treatment path.
| Tissue Type | Fat | Glandular tissue |
| Texture | Soft | Firm or rubbery |
| Pain | Rare | Sometimes tender |
| Treatment | Weight loss | Surgery or hormonal therapy |
Doctors rely on physical examination and imaging to accurately differentiate obesity from true gynecomastia.
Early diagnosis avoids frustration and ineffective treatments.
How Doctors Diagnose Obesity vs. True Gynecomastia
When evaluating Obesity vs. True Gynecomastia, doctors follow a structured diagnostic approach:
1. Clinical Examination
While the patient is lying down, doctors examine the chest. Glandular enlargement is suggested by a hard, disc-like tissue beneath the nipple.
2. Medical History
They review medication use, steroid intake, liver disease, thyroid issues, and puberty history.
3. Blood Tests
Hormonal tests measure testosterone, estrogen, thyroid levels, and liver function.
4. Ultrasound Imaging
Ultrasound helps confirm glandular tissue versus fat deposition.
5. Mammography (Rare Cases)
Used if suspicious lumps are present.
Accurate diagnosis ensures that patients receive appropriate treatment rather than relying on trial-and-error.
Treatment Options for Obesity vs. True Gynecomastia
Whether the problem is glandular or connected to obesity will determine how it is treated.
For Obesity:
- Structured weight loss programs
- Strength training and cardio
- Nutritional counseling
For True Gynecomastia:
- Hormonal correction (if early stage)
- Minimally invasive gland excision surgery
- Liposuction (if mixed tissue)
In many cases, patients may have a combination of fat and glandular tissue. Doctors customise treatment plans accordingly.
Timely intervention improves both physical appearance and emotional well-being.
Psychological Impact of Obesity vs. True Gynecomastia
Men who struggle with obesity vs true gynecomastia frequently have body image problems, social anxiety, and low self-esteem. Many avoid fitted clothes, swimming, and gym activities. Taking medical action to treat the problem boosts mental health and confidence. Expert advice removes doubt and gives patients the confidence to act.
Why Early Diagnosis Matters
Ignoring chest enlargement can exacerbate emotional suffering and postpone therapy. Untreated real gynecomastia may be a sign of underlying medical issues in cases of hormone imbalance. Early distinction between true gynecomastia and obesity avoids needless dietary frustration or postponed surgery. Medical clarity brings peace of mind and faster results.
Conclusion
Understanding the distinction between obesity and true gynecomastia is crucial for effective, lasting treatment. While obesity-related chest enlargement improves with lifestyle changes, true gynecomastia requires medical or surgical management.
Experts at Lux Hospital offer precise diagnosis, cutting-edge imaging, hormonal assessment, and customised minimally invasive surgical treatment. Lux Hospital prioritises results that seem natural, patient comfort, and safety. You can gain clarity and confidence about the difference between obesity and true gynecomastia by seeking professional advice at Lux Hospital.
Frequently Asked Questions
You can differentiate by feeling the tissue under your nipple: true gynecomastia usually presents as a firm or rubbery lump beneath the areola. In contrast, obesity-related fat feels soft and evenly distributed.
Exercise does not remove glandular breast tissue in cases of true gynecomastia, but it can help reduce total body fat and may improve chest contour in cases of obesity. Chest muscles can be developed by strength training, but the hard gland stays the same.
A hormonal imbalance between estrogen and testosterone causes true gynecomastia, which is frequently brought on by ageing, puberty, steroid use, certain drugs, or illnesses that impair hormone production. Thyroid and liver conditions might also be involved.
Gynecomastia surgery is generally safe when performed by experienced surgeons and involves removing glandular tissue through small incisions. The majority of patients heal quickly and leave little scars.
Gynecomastia rarely returns if the glandular tissue is completely removed and hormonal balance remains stable. However, steroid use or untreated hormonal disorders may increase recurrence risk.



